
CT of Blunt AbdominalTrauma in Adults
Mindy M. Horrow, MD, FACR
Director of Body Imaging
Albert Einstein Medical Center
All photos retain the copyrights of their original owners
© Mindy Horrow, MD
Background
Trauma is third most common causeof death in US
Trauma is leading cause of death in <40 years
Background
Two mechanisms for injury:
–compression- leads to solid organ & hollowviscus injury
–deceleration with stretching between moveable& fixed objects- leads to injuries ofrenal/mesenteric vessels
Technique
Multi-slice scanner
Clamp Foley, reduce artifacts (leads, arms,etc.)
If head CT needed, do before IV contrast
150 cc contrast @ 3-4 cc/sec, 70 sec delay(less if also doing chest)
Inferior lungs to inferior edge of ischia
Technique
Delayed imaging as necessary to opacifyurinary tract
Soft tissue, bone with spinereconstructions as necessary, lungwindows
“Single pass” technique- arms on bolsters@ 35-50º, scan entire body with slight delaybefore chest for IV contrast
Technique
Enteric contrast- traditionally usedoral contrast to at least opacitystomach, duodenum and proximaljejunum
–Benefit: extravasation of oral contrast is100% sensitive for bowel injury
–Risk: aspiration, delays in scanning
Stuhlfaut, Rad2004;233:689
Technique
Multi-detector CT without oral contrastmay be adequate to depict bowel andmesenteric injuries
Penetrating trauma- use of rectalcontrast
Stuhlfaut, Rad2004;233:689
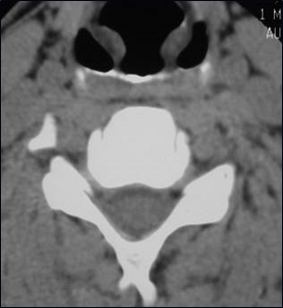
Spine
Multi-detector CT more sensitive forspine fractures than conventionalradiography. (78 vs. 32% sensitivityfor thoracic and lumbar fractures)
Wintermark, Rad2003;227:681
Spine
Reconstruct thin slices, change FOVand reformat spine images
Can replace conventionalradiography for severely traumatizedpatients undergoing imaging ofchest, abdomen and pelvis CT
Wintermark, Rad2003;227:681
Major Imaging Goals
Is surgery required?
–Hemodynamic instability
–Certain injuries
Is conservative managementlikely to fail?
–Active arterial extravasation
–Higher grades of injury
CT of Hemoperitoneum
CT can detect very small volumes offluid
Should prompt thorough search fororgan injury
Starts near site of injury andspreads by traditional pathways
Large amounts from upper abdomenmay collect in pelvis
“Sentinel clot” as marker for sourceof bleed
Extraluminal Fluid
Intra versus extra peritoneallocation
–Intra peritoneal fluid in Morrison’spouch wraps around tip of liver
–Retroperitoneal fluid in anterior para-renal space does NOT wrap aroundliver tip
Extraluminal Fluid
Intra versus extra peritoneallocation
–Extra peritoneal fluid in pre-vesiclespace extends superiorly toumbilicus

Intra peritoneal fluid
Retroperitoneal fluid
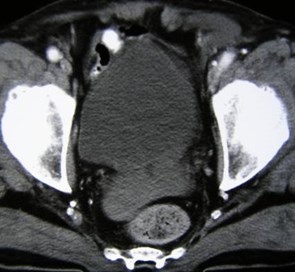
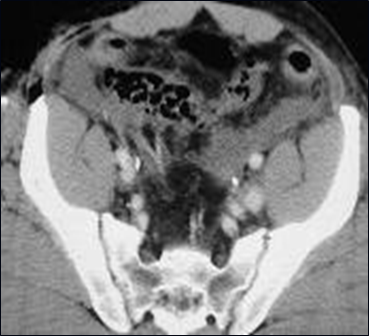
Blood in cul-de-sac and left inguinalhernia
Attenuation Valuesof Intraperitoneal Blood
> 100 HU - active hemorrhage
40-60 HU- clotted blood
30-45 HU- fresh unclottedblood
0-20 HU- serum (afterclotting)
Values can be affected by hematocrit, ascites, urine
IV contrast extravasation indicates active bleeding
Detection of AcuteHemorrhage
Various appearances: focal jet(42%), diffuse high density inhematoma (37%), focal highdensity(21%)
73% required immediate intervention
Occurred in 13% pts with blunttrauma in retrospective review of165
Exact bleeding rate unknown
Willmann, etal. AJR 2002;179:437
Acute bleeding into a mesenteric hematoma
Findings of Hypotension
Slit-like IVC, small aorta, normal colon
enhancement of spleen
enhancement adrenal glands,kidneys
Diffuse thickening of small bowel wallwith increased enhancement
Dilatation with luminal fluid
Recovery of normal bowel functionafter resuscitation
Mirvis, etal AJR 163:1375, 1994


“Shock Bowel”- shift of flow to mucosa withprolonged blood transit time
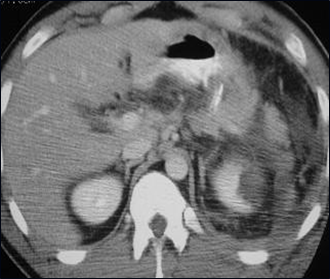
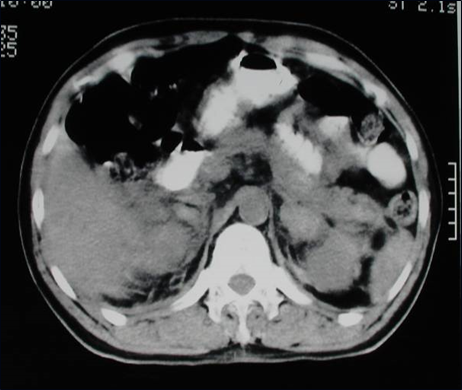
Hypodense spleen and kidneys, hyperdense adrenals

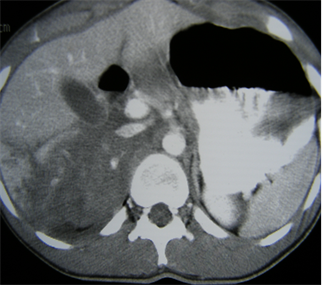
Hypodense spleen, small IVC, mucosal enhancement anddilatation small bowel
Most frequently injured abdominalorgan
~ 90% of stable patients withsplenic injury are treatedconservatively
Splenic Trauma
Surgery more likely a necessity ifCT shows large area of non-perfusion, active hemorrhage, orpseudoaneurysm
CT ~ 95% sensitive for splenicinjury
Splenic Trauma
CT Findings of Splenic Injury
Subcapsular hematoma - crescent of lowattenuation compressing parenchyma
Intrasplenic hematoma - round, lowattenuation (early), inhomogeneity, highattenuation clot (later)
Contusion - mottled parenchymalenhancement
CT Findings of Splenic Injury
Laceration - connects opposing visceralsurfaces
Shattered spleen - multiple lacerations
Associated with: hemoperitoneum, adjacentclot, thickening of lateral conal fascia
Look carefully for vascular lesions- PSA orAVF
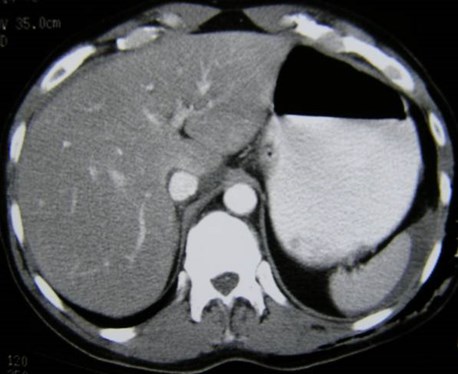
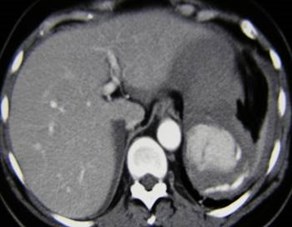
Perisplenic hematoma and homogeneous spleen, smalllaceration found at surgery for other injuries

Splenic contusions


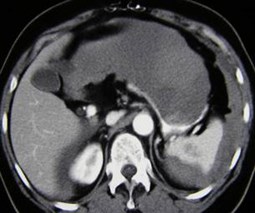
Splenic contusion with pseudoaneuryms

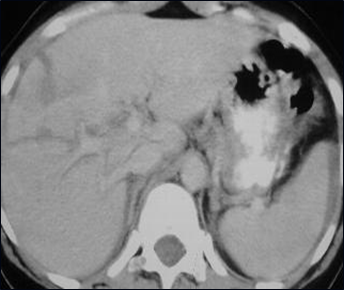
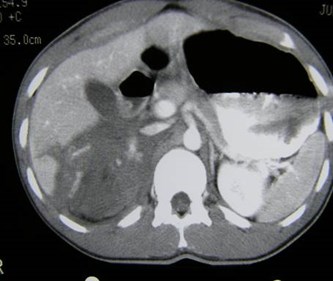
Shattered spleen with associated left
renal laceration & hemoperitoneum

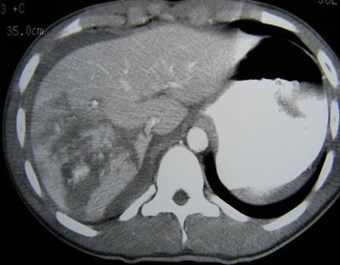
Splenic contusions, lacerations, acute hemorrhage
Pitfalls of CT in SplenicTrauma
Lobulations, congenital clefts,prominent left hepatic lobe, streak &motion artifacts
–On delayed imaging a cleft will remainhypodense because it contains fat,lacerations increase in density
Pitfalls of CT in SplenicTrauma
Inhomogeneous enhancement dueto early scanning
Differentiation of subcapsular frompericapsular peritoneal bleedingmay be difficult
Grading systems for triage havevariable success
Younger patients can tolerate verysevere injuries with conservativemanagement
Older patients (> 55 yrs) may requiresurgery for seemingly minor injuries
Outcomes after splenictrauma
CT frequently underestimates extentof injury found at surgery
Increasing grade of injury doescorrelate with length of time tohealing
Outcomes after splenictrauma
Hepatic Trauma
2nd most frequently injuredabdominal organ
Greater morbidity than spleniclaceration
~ 1/2 with liver injury also havesplenic injury
Great capacity for healing, nodelayed rupture
CT Findings of HepaticTrauma
Posterior segment right lobe mostfrequent site (near spine & ribs)
Most common lacerations areperivascular
CT Findings of HepaticTrauma
If multiple lacerations around IVCor porta, suggest hepatic veindamage
Lacerations extending to bare areamay only have retroperitonealfindings
Periportal Low Attenuation“Tracking”
Found in 22% patients withblunt abdominal trauma
Periportal Low Attenuation“Tracking”
Causes include:
–Dissecting hemorrhage
–Dissecting bile
–Dilated interlobar lymphaticsfrom CVP 2º vigorous fluidresuscitation
Lacerations - irregular, linear or roundbranching regions of low attenuation
Focal hepatic devascularization - wedges oflow attenuation extending to liver surface
Intraparenchymal hematomas - mass-like,well defined regions of low attenuation
CT Findings of HepaticTrauma
Contusions - ill defined areas of lowattenuation
Subcapsular hematomas - often withassociated rib fractures
Acute hemorrhage (80-350 HU)
Pitfalls- streak artifacts, fatty liver, masses
CT Findings of HepaticTrauma

Liver lacerations with periportal tracking andperihepatic/perisplenic hemoperitoneum

Liver lacerations with devascularizationand acute hemorrhage


CXR-subcutaneous
emphysema
CT- tiny PTX
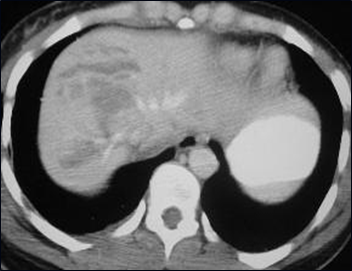

Liver lacerations & contusions
without hemoperitoneum
Delayed ComplicationsAfter Hepatic Trauma
Occur in up to 20%
Include: recurrent bleeding, AV fistula, PSA,biloma, obstructive jaundice 2º biloma
CT before discharge is more important inpatients with liver than splenic injury
As with spleen, CT grade of injury notaccurate indicator of outcome
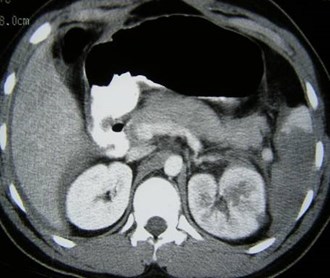
CT of Gallbladderand Biliary Trauma
Rarely injured during blunt abdominaltrauma
Gallbladder:
–Blurring, thickening or discontinuity ofwall. Usually with associated liver andduodenal injuries. Diagnosis difficultbecause signs are non-specific
Bile Ducts:
–Laceration may be partial or complete,associated 20% mortality. Mostcommon where duct exits liver or enterspancreas
CT of Gallbladderand Biliary Trauma
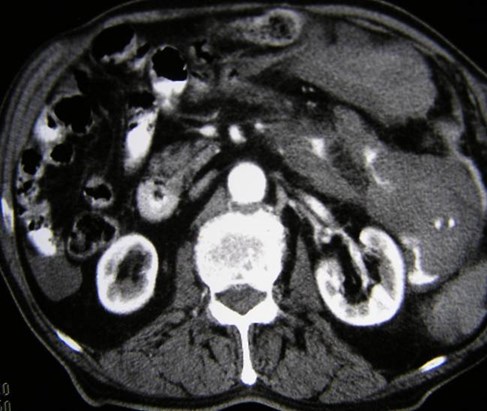
CT of Pancreatic Trauma
Rare injuries, more common inyoung adults, due to compression
Almost always associated with otherorgan injury
Delay in diagnosis leads to:recurrent pancreatitis, pseudocyst,fistula, abscess
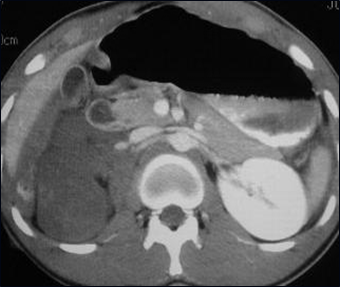
CT Findings in PancreaticTrauma
Often subtle: edema, adjacent fluid,focal or diffuse pancreatic enlargement,fluid around SMA, fluid in lesser sac orbetween pancreas and splenic vein*
–Look for asymmetry in normal pancreaticseptations
CT Findings in PancreaticTrauma
Obvious findings: fracture throughpancreatic parenchyma, irregularcontour
Major duct injury may be presentwithout any findings on initial, early CT

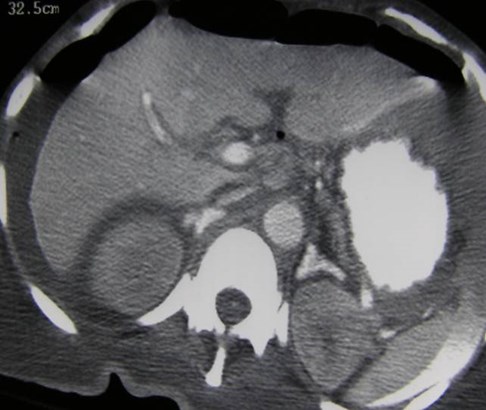
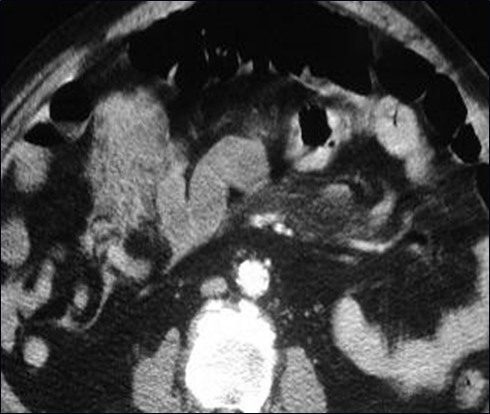
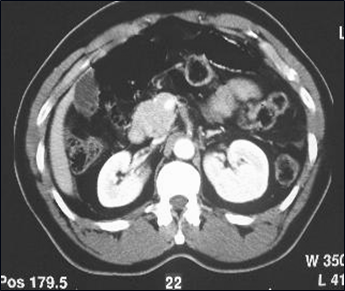
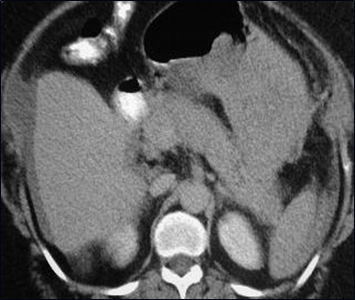
Pancreatic tail fracture with
associated left renal injury
CT of Bowel and MesentericTrauma
Occurs in 5% of patients undergoingsurgery after trauma
Signs and symptoms may be minimal
If surgery is delayed, morbidityincreases
CT of Bowel and MesentericTrauma
Especially important to detectbecause many cases of solid organinjury will not require surgerywhereas bowel/mesenteric injuriesrequire exploration
–Nghiem, etal AJR 160:53, 1993
–Rizzo, etal Radiology 173: 142, 1989
CT Findings ofBowel/Mesenteric Injury
Small Bowel: injuries of duodenum, atligament of Treitz or ileo-cecal valve
–Focal bowel wall thickening
–Free air/contrast only in 1/3
–Focal discontinuity and sentinel clot
–Pneumatosis
–Streaky increased attenuation in mesentery
–Free fluid (in absence of other organ injury)** especially triangular shaped collections
Mesenteric injuries are rarely isolated
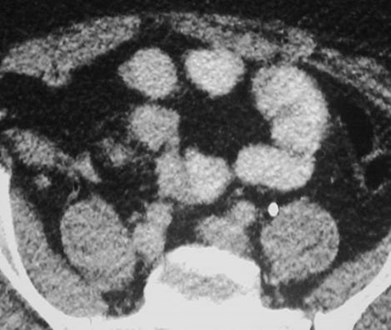
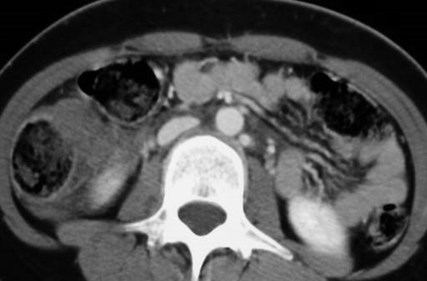
Mesenteric hematoma

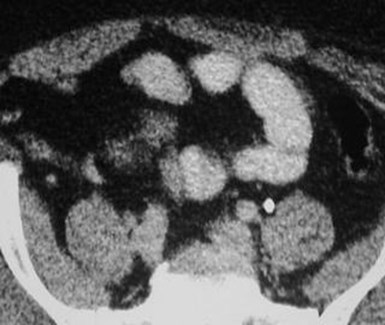
Acute mesenteric hemorrhage
With associated splenic injury
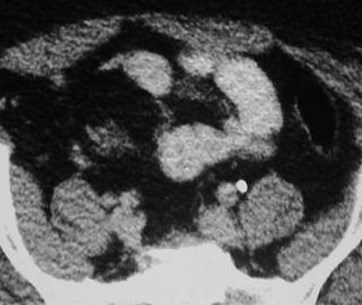
Acute mesenteric hemorrhage
Hemo-pneumo-
peritoneum
Small liver
lacerations


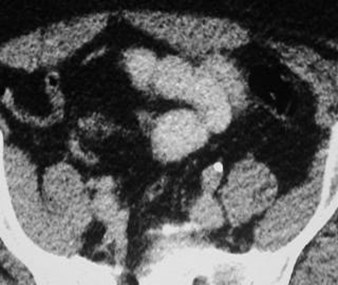
Free air

Injury to jejunum at ligament of
Treitz with sentinel clot
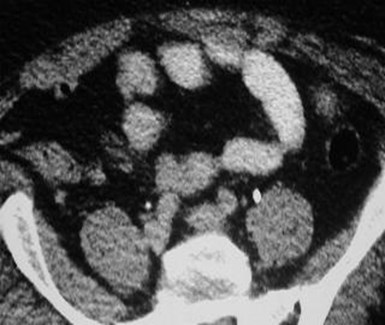
Subtle mesenteric
hematoma in an obese pt
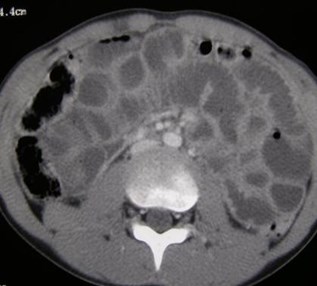
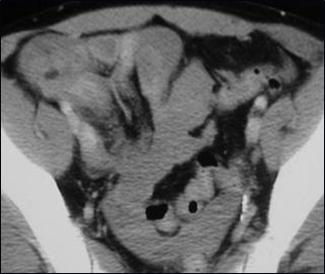
Ill defined walls of sigmoid colon withpneumatosis and sentinel clot


Disruption of enhancing colonic wall with adjacent hematoma,required hemicolectomy

Patient on Coumadin in MVA


Omental hematoma with
hemoperitoneum
Free Intraperitoneal Air inTrauma
May often occur without injury tohollow viscus
May be 2º sealed off micro-perforation, PTX, dissection ofsubcutaneous air or via femalegenital tract
Hamilton, etal J Trauma 39:331, 1995
Kane, etal Invest Radiol 26:574, 1991
Free Intraperitoneal Air inTrauma
Use of oral contrast with delayedimaging & rectal contrast to ruleout bowel perforation
Hamilton, etal J Trauma 39:331, 1995
Kane, etal Invest Radiol 26:574, 1991
CT of Bladder Injuries
70% associated with pelvic fractures
Add on CT cystogram if bladder isnot distended at time of initial scan
1. ~ 350 mL of 5% contrast materialinstilled via Foley
2. Evaluate urethra before Foleyplacement as necessary
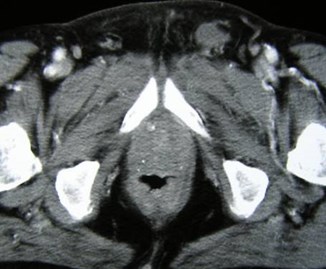
CT Findings of Bladder Injuryon Cystogram
Contusion - focal thickening, variableattenuation
Rupture - extravasation
1.Extraperitoneal - peri/prevesical,anterior abdominal wall, thigh, penis,scrotum
2.Intraperitoneal - pericolic gutters,around bowel loops, pouch of Douglas

Pelvic fractures- negative cystogram
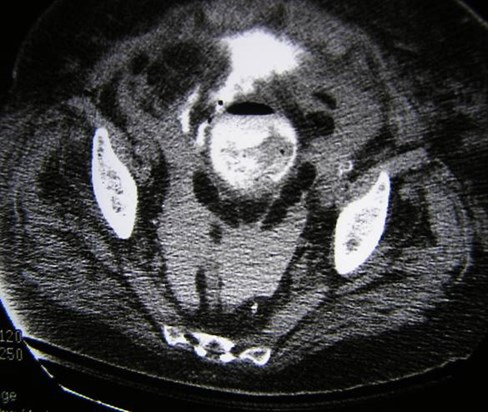
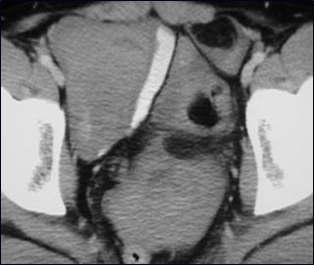
Intra and extra peritoneal bladder rupture
CT of Renal Trauma
Injury is common but 95% minor
Hematuria in 95% with renal trauma
Renal pedicle or vein injury may haveno hematuria
Initial imaging @ 70-80 sec for vascularenhancement and nephrogram
Delayed images (3-5 min) to check forurine leak
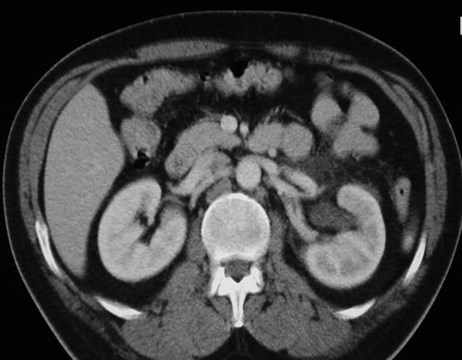
CT Findings of Renal Injuries
Contusions: patchy areas of decreasedenhancement, striated nephrogram
Lacerations: irregular, linear, low-attenuation
Fracture: a laceration through hilum
Subcapsular hematoma: low attenuationcrescent, compressing parenchyma
Arterial injuries: main, segmental
Venous injuries: persistent nephrogram



Initial
Delayed
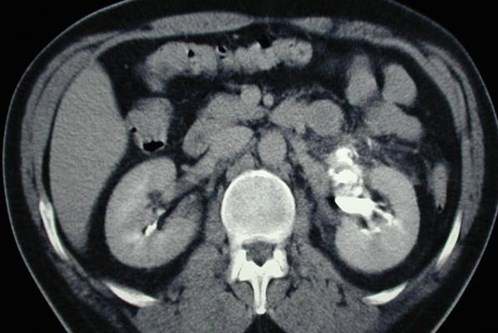
Renal fracture:
Involving renal pelvis with urineextravasation and retroperitonealhematoma



Renal fracture with
hematoma:
initial imaging
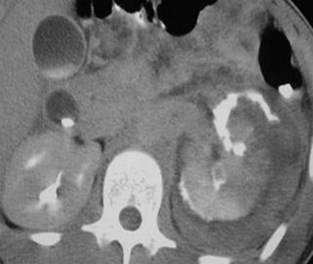
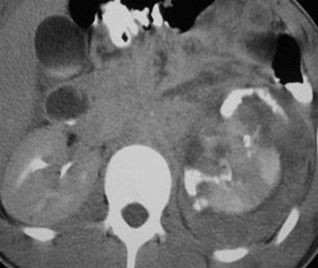
Injury to collecting system
with extravasation
Delayed imaging
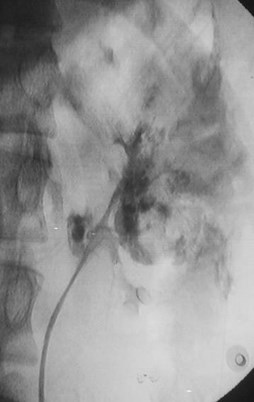
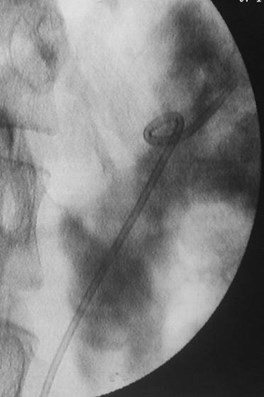
Retrograde study, stent placement


IVU several weeks later with healed, intactcollecting system
nephrogram
pyelogram
Initial image with slightly delayed left
nephrogram, perinephric fluid and partial renal veinthrombus
Renal pelvis injury with leak of urine
Delayed imaging
Renal pedicle injury
Involving artery and vein
With hematoma

Initial study One day later
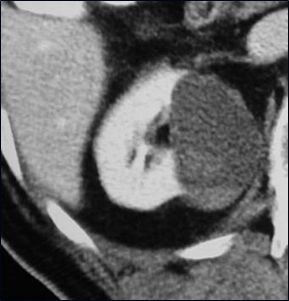
Hemorrhage into renal cyst
Adrenal Trauma
Adrenal injuries in 2% of thoseundergoing CT
Hematoma (obscured gland),active extravasation
May need follow-up to rule out atrue adrenal mass
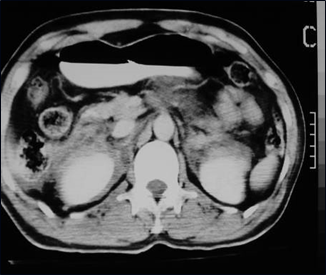

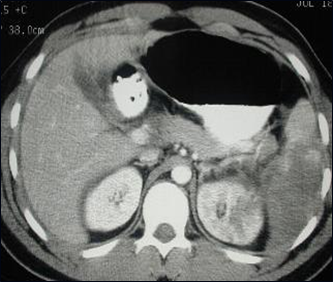
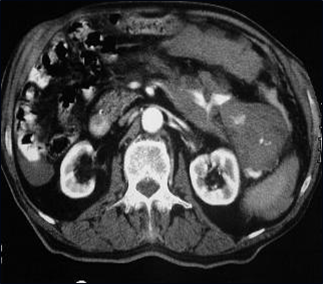
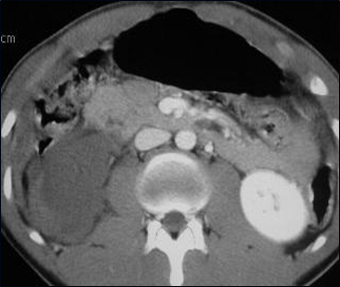
Day 1- Bilateral adrenal hemorrhages causing smallperinephric hematomas
Day 2- adrenal hemorrhages without
IV contrast
Acute extravasation from right adrenal gland in patientwith major hepatic injury
Miscellaneous Trauma
Chest injuries detected on upperabdominal images
Diaphragm- 1-2 % incidence,bowelin chest, disruption in diaphragm,variable sensitivity & specificity
Vessels
Extra-abdominal injuries- occur inup to 75% with major abdominaltrauma

Pneumothorax
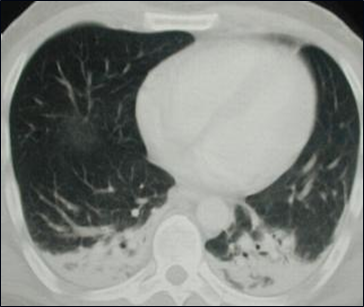
Aspiration pneumonia

Acute hemorrhage into soft tissues
Vascular Injuries
Irregular contour,indistinct borders,intimal flap,extravasation
IVC injury often 2ºliver laceration, mayneed femoral veininjection to opacifyIVC and confirminjury

Traumatic aorta dissection, peri-aortic blood



Multi-trauma
Rib
Liver
Spleen
Spine


Multi-trauma
Duodenal hematoma with acute hemorrhage



Multi-trauma
Ileal hematoma
Sacral fracture
Conclusions
CT is imaging study of choice inabdominal trauma
Multislice technology permits rapidimaging and multiple scans asneeded
Novelline, etal. RadClinicsNA, 1999;37:3, 591
Conclusions
Combined studies with single bolus
2D and 3D reformations usefulespecially for spine
Increasing use in penetrating trauma
Novelline, etal. RadClinicsNA, 1999;37:3, 591
The End